Guidelines for using
Blue Light Cystoscopy with Cysview®
Blue Light Cystoscopy (BLC®) with Cysview is included in Canada, US, and international industry guidelines.
CUA Guidelines (2021):1
Patients presenting with a bladder tumour should undergo initial TURBT for diagnostic confirmation and pathological evaluation.
TURBT optimization: when available blue light cystoscopy (BLC) can increase tumor detection at first TURBT and reduce recurrence risk.
The quality of the initial TURBT is of utmost importance.
AUA/SUO Guidelines (2016, Amended 2020):2
In a patient with NMIBC, a clinician should offer BLC at the time of TURBT, if available, to increase detection and decrease recurrence. (Moderate Recommendation; Evidence Strength: Grade B)
Diagnosis
At the time of resection of suspected bladder cancer, a clinician should perform a thorough cystoscopic examination of a patient’s entire urethra and bladder that evaluates and documents tumor size, location, configuration, number, and mucosal abnormalities. (Clinical Principle)
At the initial diagnosis of a patient with bladder cancer, a clinician should perform a complete visual resection of the bladder tumor(s), when technically feasible. (Clinical Principle)
A clinician should perform upper urinary tract imaging as a component of the initial evaluation of a patient with bladder cancer. (Clinical Principle)
In a patient with a history of NMIBC with normal cystoscopy and positive cytology, a clinician should consider prostatic urethral biopsies and upper tract imaging, as well as enhanced cystoscopic techniques (blue light cystoscopy, when available), ureteroscopy, or random bladder biopsies. (Expert Opinion)
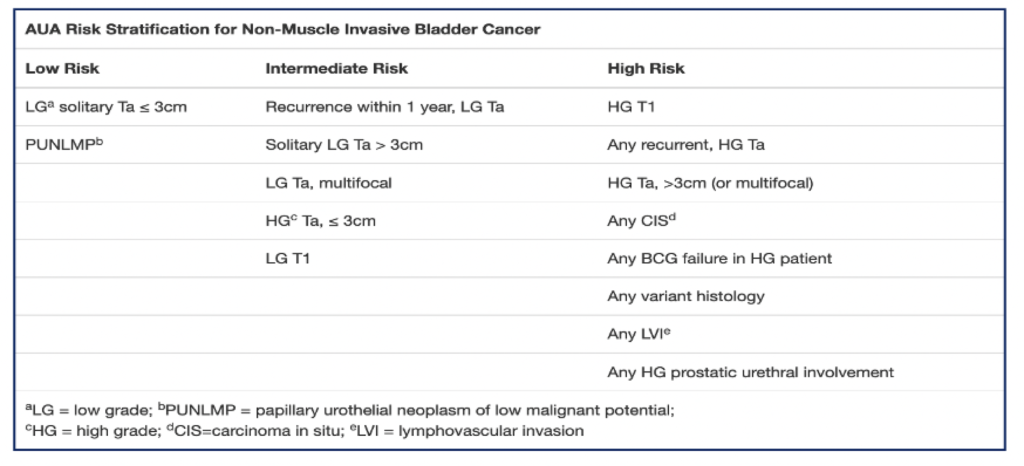
Risk stratification
At the time of each occurrence/recurrence, a clinician should assign a clinical stage and classify a patient accordingly as “low-,” “intermediate-,” or “high-risk.” (Moderate Recommendation; Evidence Strength: Grade C)
US Consensus Statement:3
Blue Light Cystoscopy with Cysview should be used “at initial TURBT on suspicion of NMIBC.”
BLC with Cysview increases tumour detection, which improves intra-operative4 and post-operative5 disease management.
References:
Witjes JA, Babjuk M, Gontero P, et al. Clinical and Cost Effectiveness of Hexaminolevulinate-Guided Blue-Light Cystoscopy: Evidence Review and Updated Expert Recommendations. Eur Urol. 2014;66(5):863-871.
Bhindi B, Kool R, Kulkarni GS, et al. Canadian Urological Association Guideline on the Management of Non-Muscle-Invasive Bladder Cancer – Full-Text. Can Urol Assoc J 2021;15(8): E424-457.
Chang SS, Boorjian SA, Chou R, et al. Diagnosis and Treatment of Non-Muscle Invasive Bladder Cancer: AUA/SUO Guideline. J Urol. 2016;196(4):1021-1029.
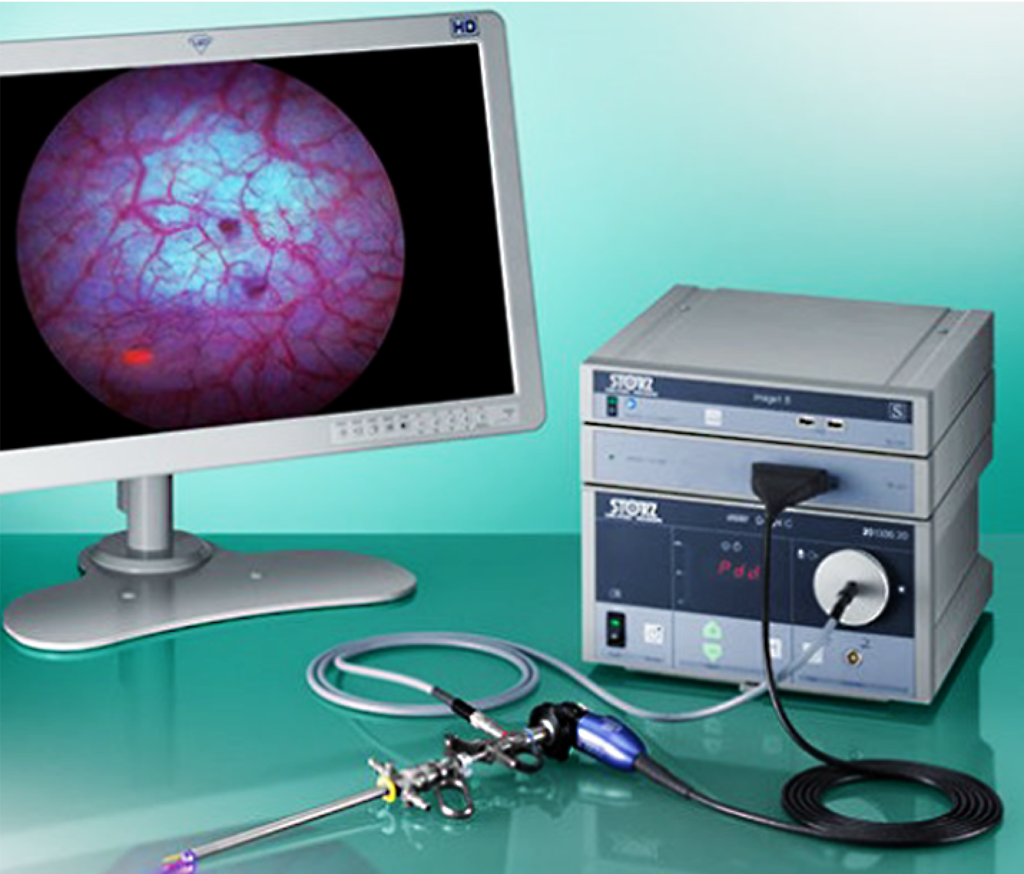
Required Equipment
Approved cystoscopic equipment with necessary filters to allow both White Light Cystoscopy (WLC) and Blue Light Cystoscopy (BLC®) is available in Canada through two manufacturers: KARL STORZ and RICHARD WOLF.
KARL STORZ was the first to provide BLC equipment in Canada. The IMAGE1 S™ Saphira™ system includes a camera-control-unit with camera head and resectoscope with a special light source that supports use of both white and blue light.
RICHARD WOLF launched its System Blue equipment in 2023. Visualization includes white light mode, bluePDD SIM mode, and bluePDD Color Contrast SIM mode. The camera head generated 4K UHD resolution.
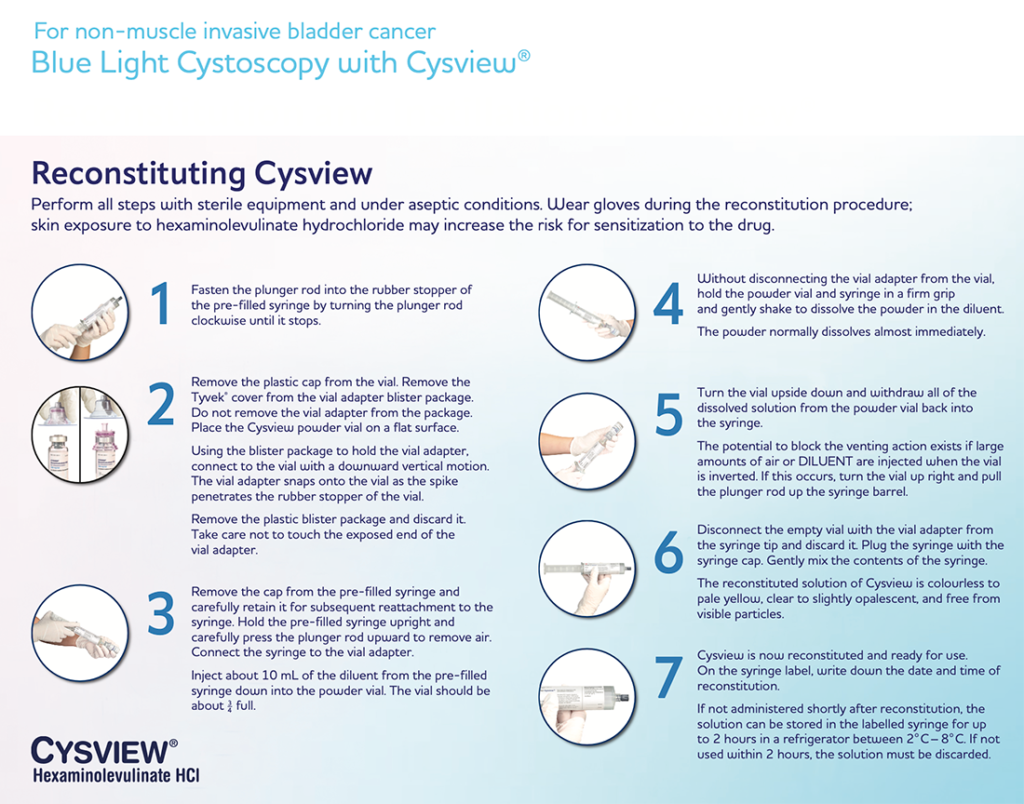
Reconstitution and Instillation
A Step-By-Step Guide to the Reconstitution and Instillation of Cysview Using the Pre-filled Syringe
This video walks you through the steps of Cysview reconstitution and instillation.
For non-muscle invasive bladder cancer Blue Light Cystoscopy with Cysview
This Reconstitution and Instillation guide provides step-by-step instructions for reconstituting and instilling Cysview
Use Blue Light Cystoscopy (BLC®) with Cysview in patients with non-muscle invasive bladder cancer (NMIBC).
Use in first TURBT and the management of intermediate and high-risk patients.
Consider for patients:
At initial TURBT on suspicion of NMIBC
Having repeat TURBT
Being checked to assess response to BCG therapy 6 weeks after completion
Undergoing surveillance
Prior to intravesical therapy when the residual disease is suspected, and the patient has not previously had BLC with Cysview
With positive cytology and negative White Light Cystoscopy (WLC)
Guideline and expert consensus recommendations
At initial TURBT on suspicion of NMIBC
AUA/SUO Guideline:
In a patient with NMIBC, a clinician should offer BLC with Cysview, if available, to increase detection and decrease recurrence. (Moderate Recommendation; Evidence Strength: Grade B).1
From Pivotal Clinical Study:
In a prospective, comparative, within-patient controlled, multicenter phase III study in the detection of Ta/T1 tumors in patients who had previously undergone a cystoscopy and had suspicion of or confirmed NMIBC: Out of 286 patients with at least one Ta or T1 tumor, 16% were detected only with BLC with Cysview (p=0.001).2
2018 Consensus Panel of NMIBC experts:
Strong recommendation to use BLC with Cysview.3
During Repeat TURBT
2018 Consensus Panel of NMIBC experts:
BLC with Cysview is strongly recommended in intermediate and high-risk patients.
Following treatment with BCG
2018 Consensus Panel of NMIBC experts:
The decision to use BLC with Cysview in this instance should be made on a patient-by-patient basis by taking into account the benefit from accurately diagnosing more clinically significant disease cases versus the risk of false positives. The incidence of false positives decreases as time from BCG therapy increases.4
2018 Consensus Panel of NMIBC experts:
This scenario is an important endpoint for BLC with Cysview in high-risk patients.3
In surveillance
2018 Consensus Panel of NMIBC experts:3
For intermediate-risk patients
At HCP-determined frequency during surveillance for 2 years
For high-risk patients
At every other follow-up for 2 years
Prior to intravesical therapy when residual disease is suspected when the patient has not previously had BLC® with Cysview®
2018 Consensus Panel of NMIBC experts:
A majority of the panel (13/17) thought that BLC with Cysview would be of benefit before initiating intravesical therapy in patients at intermediate risk or high risk of recurrence, based on the patient’s not having undergone a previous TURBT using BLC with Cysview.3
When positive cytology and negative WLC
AUA/SUO Guideline:
In patients with a positive cytology and negative WLC, a clinician should consider prostatic urethral biopsies and upper tract imaging, as well as enhanced cystoscopic techniques (BLC, when available), ureteroscopy, or random biopsies. (Expert Opinion).1
References:
Chang SS Boorjian SA, Chou R, et al. Diagnosis and Treatment of Non-Muscle Invasive Bladder Cancer: AUA/SUO Guideline. J Urol. 2016;196(4):1021–1029. Amended 2020.
Stenzl A, Burger M, Fradet Y, et al. Hexaminolevulinate Guided Fluorescence Cystoscopy Reduces Recurrence in Patients with Nonmuscle Invasive Bladder Cancer. J Urol. 2010;184(5):1907–1914.
Lotan Y, Bivalacqua TJ, Downs T, et al. Blue Light Flexible Cystoscopy with Hexaminolevulinate in Non-Muscle Invasive Bladder Cancer: Review of the Clinical Evidence and Consensus Statement on Optimal Use in the USA—Update 2018. Nat Rev Urol. 2019;16(6):377–386.
Daneshmand S, Schuckman AK, Bochner BH, et al. Hexaminolevulinate Blue-Light Cystoscopy in Non-Muscle Invasive Bladder Cancer: Review of the Clinical Evidence and Consensus Statement on Appropriate Use in the USA Nat Rev Urol. 2014;11(10):589–596.
Expert Tips and Experience with Cysview®
Observation
Cause
Solutions
Visual
Weak Fluorescence
Equipment failure or
Blood in the bladder or
Inadequate time or
Air bubbles or
Concealed tumours
Make sure equipment is working and connected properly
If blood is present, remove resectoscope and flush using a bladder syringe attached to the trocar
Ensure that Cysview was instilled 1 hour prior to cystoscopy
Remove any air bubbles
Look behind any folds
No fluorescence
The equipment has not been set up correctly
Blue Light is not activated
No malignant activated lesions
Ensure you are using correct equipment; look for blue or violet marker
Make sure Cysview has been instilled, and check for fluorescence in bladder neck
Inspect light source; original light bulb?
Green Hue
Urine in the bladder
Always drain the bladder at start of the procedure
Remove resectoscope, set trocar valve to exit position, and allow urine to drain passively
Entire bladder appears red under white and blue light
Recent Bacillus Calmette-Guerin treatment or inflammation
If clinically feasible, avoid BLC with Cysview until 6 weeks after last BCG treatment and in patients with bladder infection
Either continue procedure without the benefit of Blue Light diagnosis or reschedule
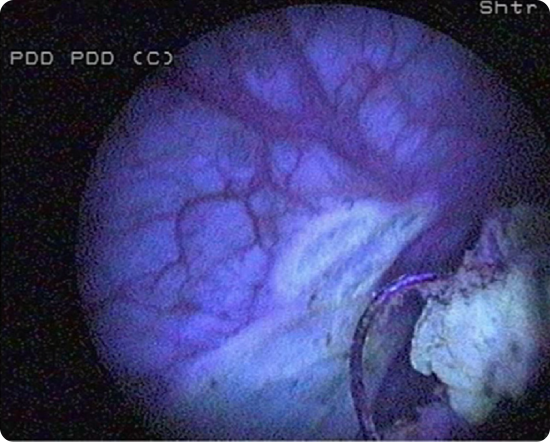
Photo Bleaching
Prolonged use of blue light
Blue light too close to lesion during procedure
Alternate between white light and blue light. If the tumour is visible in white light, use BLC with Cysview for control after resection
Do not use Blue Light close to the tumour for extended time periods. If photo bleaching appears, shut off the blue light and work elsewhere
Mark small lesions early during procedure
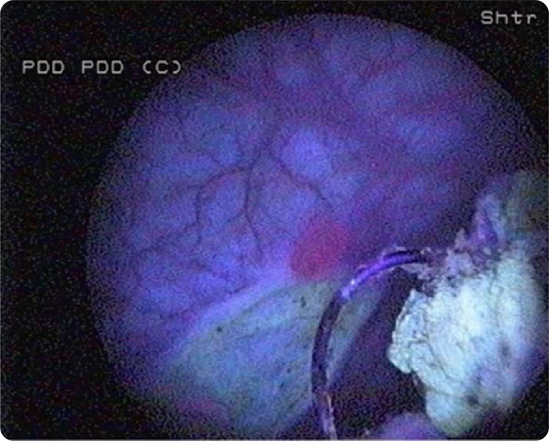
Uncertainty around a large pink/ red area
Direct scope 90° toward lesion. Fill bladder slightly. Stretch area with loop and see if it disappears
Questions:
Has a cytology been taken? Were bacterial cultures taken? Has patient used catheter for longer periods?
Is CIS suspected? Cold cup biopsy and no fulguration
Did the patient have a positive urine cytology? Treat as carcinoma in situ
Trouble finding orifice or suspicion that orifice might have been resected
Switch to Blue Light and wait in suspected area; you might see a green cloud emerging because urine appears fluorescent green under blue light
Observation
Cause
Solutions
Visual
Weak Fluorescence
Equipment failure or
Blood in the bladder or
Inadequate time or
Air bubbles or
Concealed tumours
Make sure equipment is working and connected properly
If blood is present, remove resectoscope and flush using a bladder syringe attached to the trocar
Ensure that Cysview was instilled 1 hour prior to cystoscopy
Remove any air bubbles
Look behind any folds
No fluorescence
The equipment has not been set up correctly
Blue Light is not activated
No malignant activated lesions
Ensure you are using correct equipment; look for blue or violet marker
Make sure Cysview has been instilled, and check for fluorescence in bladder neck
Inspect light source; original light bulb?
Green Hue
Urine in the bladder
Always drain the bladder at start of the procedure
Remove resectoscope, set trocar valve to exit position, and allow urine to drain passively
Entire bladder appears red under white and blue light
Recent Bacillus Calmette-Guerin treatment or inflammation
If clinically feasible, avoid BLC with Cysview until 6 weeks after last BCG treatment and in patients with bladder infection
Either continue procedure without the benefit of Blue Light diagnosis or reschedule
Photo Bleaching
Prolonged use of blue light
Blue light too close to lesion during procedure
Alternate between white light and blue light. If the tumour is visible in white light, use BLC with Cysview for control after resection
Do not use Blue Light close to the tumour for extended time periods. If photo bleaching appears, shut off the blue light and work elsewhere
Mark small lesions early during procedure
Uncertainty around a large pink/ red area
Direct scope 90° toward lesion. Fill bladder slightly. Stretch area with loop and see if it disappears
Questions:
Has a cytology been taken? Were bacterial cultures taken? Has patient used catheter for longer periods?
Is CIS suspected? Cold cup biopsy and no fulguration
Did the patient have a positive urine cytology? Treat as carcinoma in situ
Trouble finding orifice or suspicion that orifice might have been resected
Switch to Blue Light and wait in suspected area; you might see a green cloud emerging because urine appears fluorescent green under blue light
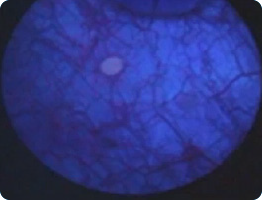
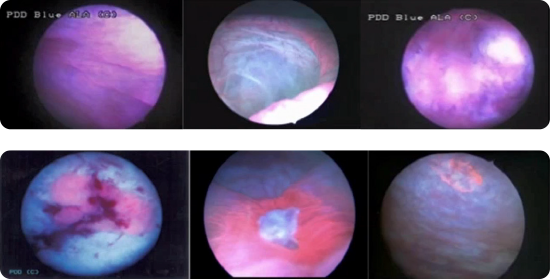
Resection Management with Blue Light
To avoid false-negative diagnoses
Ensure adequate time after instillation of Cysview
Pink fluorescence on bladder neck should always be seen if the instillation was administered properly
Bladder neck
Fluorescence is considered normal and not necessarily tumour
Want to learn more?
If you’d like more information about how and when to use Cysview, trouble-shooting tips, or anything else, request a visit from your Photocure Key Account Manager. Contact Us